Adapted by Claudio López Bruzual, MD.

Performing tests that meet the criteria indicated by the American Thoracic Society (ATS) allows adequate patient care.
It never hurts to recall the matters that we already take for granted in practice, we shall now give a brief review of what the before mentioned association considers acceptable.
Acceptability criteria
The American Thoracic Society has published guidelines in which it is defined whether the patient has made a maximum effort and, if therefore,the measurements of FEV1 and FVC obtained are adequate (acceptability criteria of the maneuver). Let us remember the maneuvers and the acceptable values.
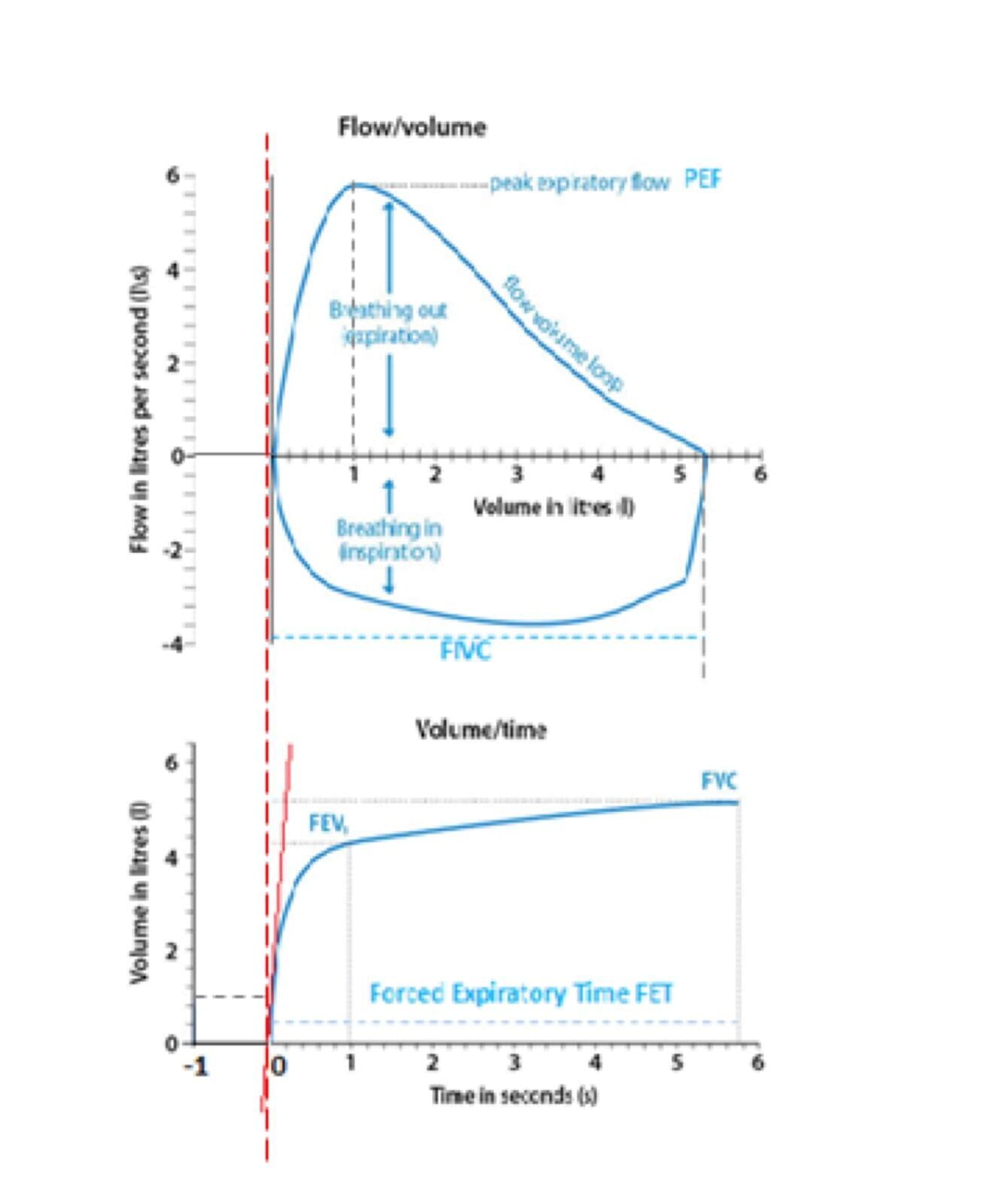
1 The beginning of the forced expiration maneuver to establish the duration of the same is determined by the method of BACK EXTRAPOLATION.
In the image below, we can see that by drawing a tangent to the lower curve at the point of the Peak Expiratory Flow (PEF), which corresponds to 1 lt in the image, we define time 0. If we raise a perpendicular line from the beginning of the lower curve (before 0) we define a volume of air before 0 in the lower curve, in this case 0.1 lts. Note the small difference between the red dotted line and the "Y" axis (the vertical line) on the top curve.
That small difference defines a volume on the "X" axis (the horizontal line). In the image, that is the BEV (Back Extrapolated Volume), in other words, the volume of gas that has already been exhaled from the forced inspiration before reaching time 0 and appears reflected in the measurements of the Spirometers together with the FEV1 and the FVC. The BEV acceptability limit must be <5% of the FVC or 0.100 lts (the used value is the highest).
2 The pause between the forced inspiration and the beginning of expiration (time 0 as defined above) should be not greater than 2 seconds.
- There must be an expiratory PLATEAU as defined by a volume change of <0.025 lts for at least 1 second on the volume time curve. The system used to perform spirometry must have an indicator of compliance with this criterion.
- The patient reaches a Forced Expiratory Time (FET) of 15 seconds. The system used to perform spirometry should provide an indicator to recognize that this goal was achieved.
- The Forced Vital Capacity is within the tolerance limits for repeatability: the difference between the two highest FVC values must not be greater than 0.100 lts, or the two highest values must not be separated by more than 10%.
Finally, we must consider that:
- Coughing during the first second of the expiratory maneuver makes FEV1unacceptable and cannot be used. However, the FVC may be acceptable.
- The closure of the glottis or the early termination of the expiratory maneuver (as with the onset of inspiration or the patient taking the mouthpiece out of the mouth) make FVC unacceptable. If any of this occurs within the first second of expiration, FEV1is unacceptable and therefore not usable.
- There should be no loss of air around the patient's mouth, nor obstruction of the mouthpiece.